

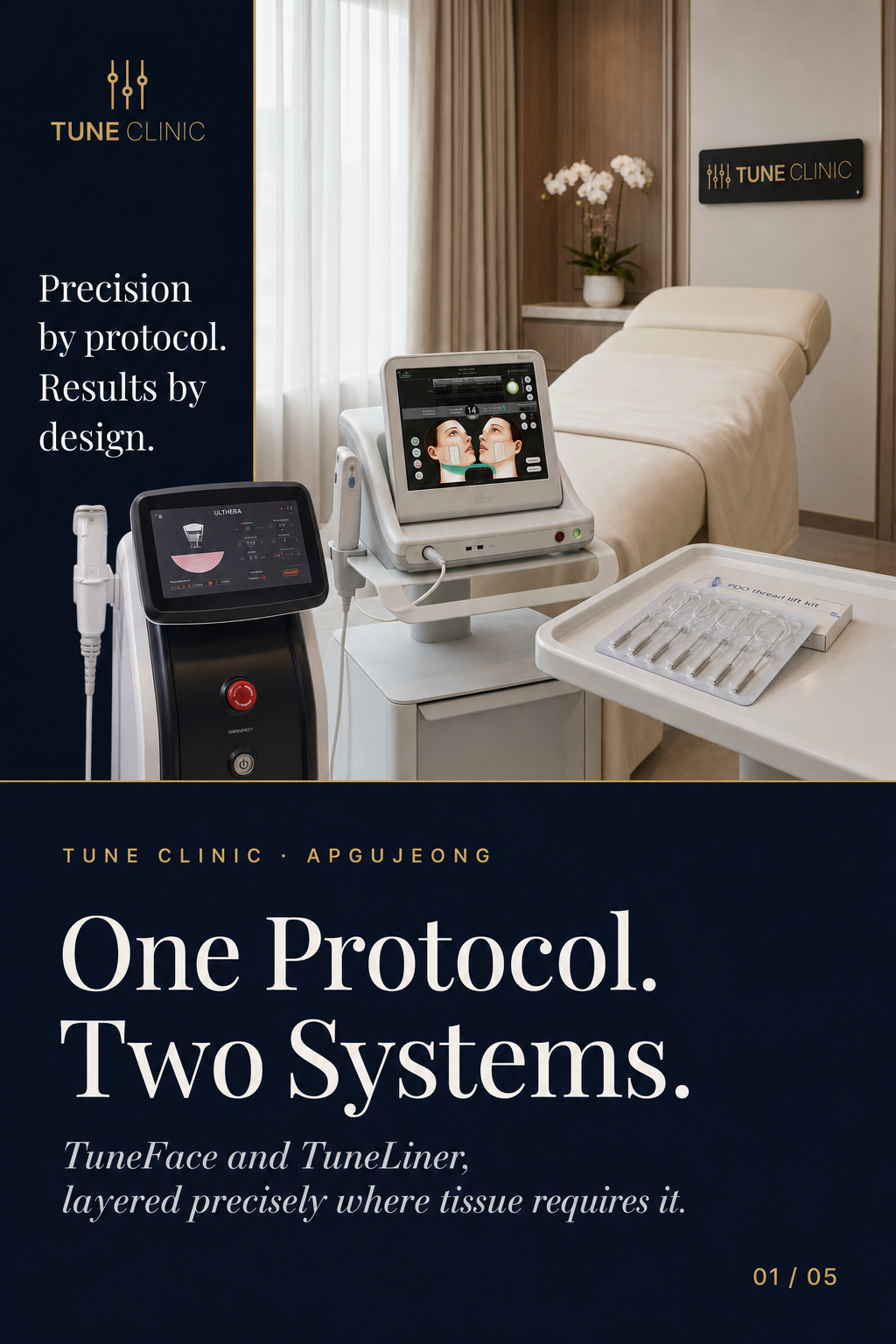

TuneFace and TuneLiner are two distinct lifting protocols that work across different tissue depths and facial zones — Ultherapy and monopolar radiofrequency addressing deeper structural laxity in the mid-face, PDO thread placement targeting vector correction along the mandibular line. Used together in a single sequenced plan, they allow a physician to assign each modality only to the tissue layer it can structurally influence, rather than applying one device broadly and hoping adjacent zones respond.
Why Single-Depth Lifting Protocols Fall Short
Most patients presenting with visible facial laxity are experiencing change at several anatomical levels simultaneously: ligament elongation, soft tissue descent, early bone resorption, and dermal thinning do not progress at the same rate or respond to the same stimulus. A protocol that delivers energy at one depth — say, focused ultrasound to the SMAS — may produce real structural tightening without meaningfully addressing mandibular blurring driven by ptotic jowl fat and lax retaining ligaments. Conversely, thread placement that corrects a jawline vector does nothing for the flattened mid-cheek that makes the correction look incomplete.
The practical consequence: a result that appears technically successful in isolation but reads as incomplete in the mirror.
“The question is never which modality is best. It is which modality belongs at which depth, in which zone, at which point in the sequence. That is a mapping problem before it is a treatment problem.”
What Does TuneFace Actually Target?
TuneFace is the clinic’s mid-face lifting protocol, built around Ultherapy Prime and Oligio (monopolar radiofrequency). These two modalities address different depth planes but share a common goal: stimulating structural collagen remodeling in tissue that has lost mechanical integrity.
Ultherapy Prime delivers micro-focused ultrasound energy to the SMAS and deep dermis. The depth and spacing of each transducer line is guided by real-time imaging, which allows the treating physician to visualise the tissue plane before committing energy. This matters in the mid-face, where fat compartment boundaries and ligament positions vary meaningfully between patients.
Oligio, as a monopolar radiofrequency device, heats a broader column of tissue from the dermis downward — a different mechanism to ultrasound and a different depth profile. Used after Ultherapy in the same session or as a standalone maintenance treatment, it contributes to dermal thickening and tightening in the overlying soft tissue that ultrasound energy alone does not fully reach.
The combination is not about redundancy. It is about covering depths that no single modality spans completely.
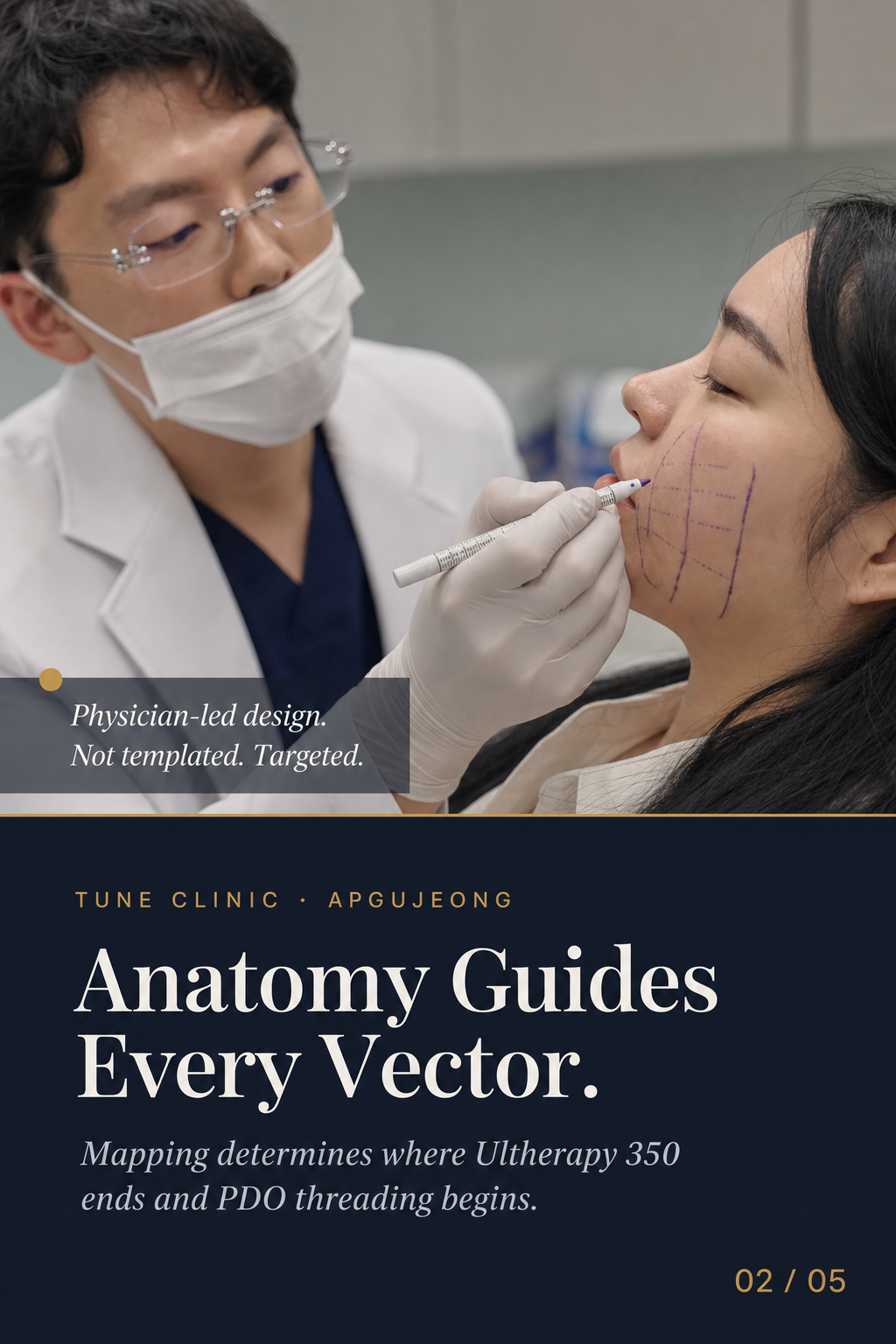
How Anatomy Guides the Mapping
Before any energy is delivered, the physician maps the face — identifying where volume loss is contributing to apparent laxity versus where true tissue descent is driving the concern. These are different problems that can look similar at first glance. Volume loss in the anterior cheek creates shadowing that mimics descent; actual ligamentous laxity creates jowling that filler cannot correct. Misreading one for the other produces results that look off even when the technique is flawless.
What Does TuneLiner Target?
TuneLiner is the clinic’s thread-based protocol, using PDO (polydioxanone) threads placed along precise vectors to mechanically reposition tissue and stimulate collagen along the mandibular line and lower face. Thread coagulation and the fibrotic response around the thread create a scaffold that resists the downward pull of gravity on soft tissue.
The mandibular line is a specific anatomical challenge. Jowl formation is driven partly by descent of the buccal fat pad and partly by loss of definition at the mandibular border itself. Thread vectors placed in response to this anatomy — rather than along a generic lift line — produce a jaw contour that looks restored rather than simply pulled.
PDO threads at this depth do not replicate what Ultherapy or Oligio achieve. They operate mechanically rather than thermally, and their effect is immediate (vector correction) as well as delayed (collagen induction). The immediate mechanical component is what makes them useful in a layered protocol: Ultherapy and RF address deeper remodeling that takes weeks to months to materialise; thread placement provides earlier visible definition while the deeper structural work matures.
How the Two Protocols Are Sequenced
The sequencing of TuneFace and TuneLiner within a treatment plan — whether in a single session or across staged appointments — is determined by the physician based on the degree of laxity, tissue quality, and the patient’s recovery tolerance. Several principles guide that decision:
- Energy before threads. Delivering radiofrequency or ultrasound energy after thread placement risks displacing the threads or altering the intended coagulation response. Sequencing energy-based treatments first preserves thread position and allows both modalities to act on undisturbed tissue planes.
- Zone specificity. TuneFace mapping concentrates on the mid-cheek, zygoma, and periorbital area. TuneLiner mapping focuses on the mandibular border and lower jowl. Overlap is minimal by design.
- Staged versus same-session. For patients with significant laxity, staging the protocols across two appointments allows recovery between energy delivery and thread placement and gives the physician a more accurate read of the tissue response before the second modality is applied.
For patients who qualify, combining both protocols in a single plan — with appropriate sequencing — produces a result that addresses mid-face volume loss and mandibular drift as the distinct anatomical problems they are, rather than as a single “ageing face” concern.
Learn more about the physician-led design approach that underpins both protocols at /design-method.html, or review the lifting device options in more detail at /the-tuning.html.
FAQ
What is the difference between TuneFace and TuneLiner?
TuneFace is an energy-based mid-face lifting protocol using Ultherapy Prime and Oligio (monopolar radiofrequency) to address laxity and collagen loss at the SMAS and dermal levels. TuneLiner is a thread-based protocol using PDO threads placed along the mandibular line to mechanically reposition tissue and define the jawline. The two protocols target different anatomical zones and different tissue depths, and are frequently combined in a single lifting plan.
Can TuneFace and TuneLiner be done in the same session?
For some patients, yes — though the physician will assess tissue quality, degree of laxity, and recovery tolerance before recommending a combined single-session plan versus a staged approach. When both are done together, energy-based treatments are performed before thread placement to avoid disrupting thread position or altering the coagulation response.
How long does it take to see results from a layered lifting protocol?
Thread placement produces an immediate mechanical vector correction that is visible within days. The collagen remodeling stimulated by Ultherapy and monopolar radiofrequency develops gradually, with results typically continuing to improve over several months as the deeper structural response matures. The full combined result of a layered protocol is generally assessed at around three to six months.
Is this protocol suitable for all skin types and ages?
The appropriateness of TuneFace, TuneLiner, or both depends on the individual anatomy — specifically the degree and type of laxity, tissue thickness, and whether volume loss is contributing to the apparent concern. In some patients, injectable volume restoration may be indicated before or alongside energy-based lifting. A physician consultation and facial mapping session is the starting point for any layered plan.
Do PDO threads from TuneLiner require downtime?
Most patients experience mild swelling and occasional bruising at thread entry points for several days. Strenuous activity and significant facial manipulation are typically restricted for a short period after placement. The treating physician will give specific post-procedure guidance based on the number and placement depth of the threads used.
Ready to plan your treatment?
Tune Clinic Apgujeong offers English-language consultations with Dr. Ju and Dr. Cha — a structured assessment, not a sales call.
→ Book an appointment to pick a time that fits your Seoul itinerary.
→ Message us on WhatsApp to ask in English before you commit.
