

On this page
Nasolabial folds and the forehead require filler placed at opposite anatomical depths — the nasolabial zone is treated primarily within the subcutaneous fat compartments, while the forehead demands periosteal or deep sub-muscular placement to avoid compressing the vessels that run just above the bone. Most filler complications in these two areas trace back not to product choice but to depth miscalculation. Understanding why the anatomical logic is inverted between them is the clearest way to evaluate whether a filler plan is sound.
Why Does Nasolabial Filler Depth Matter So Much?
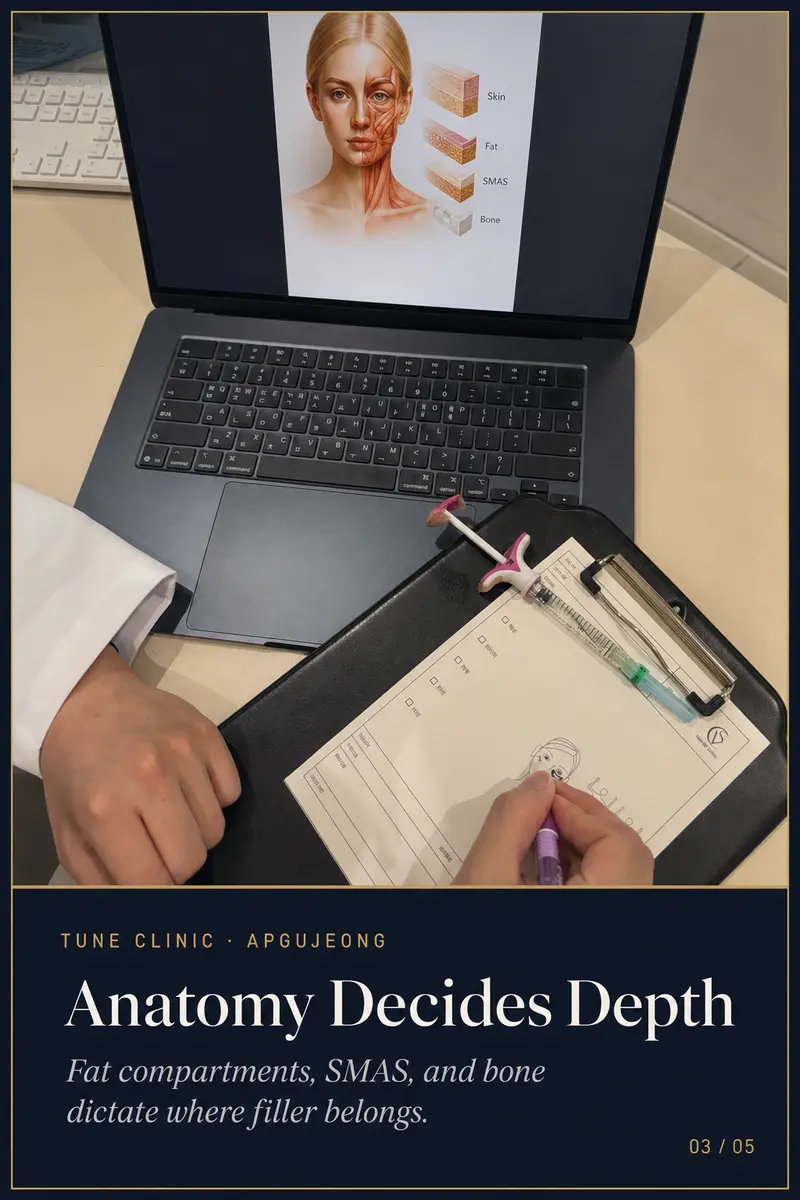
The nasolabial fold is bordered by distinct fat compartments — the nasolabial fat medially and the deep medial cheek fat laterally. When these compartments deflate with age, the fold deepens and the overlying skin loses support. The instinct to inject directly into the fold is understandable, but it is frequently wrong.
Superficial placement into the fold itself can flatten it temporarily while actually stiffening the tissue and distorting natural movement. Over time, this approach tends to make the face look heavier and more treated, not more rested. The more anatomically coherent approach addresses the volume deficit in the underlying fat compartments and, where appropriate, the pyriform fossa — restoring the structural support that causes the fold to soften as a consequence, rather than filling the groove as a target.
Depth also carries a vascular consideration. The facial artery runs a variable course in this region, and injections that stray too deep medially or too superficial laterally carry real risk. Cannula technique reduces — though does not eliminate — the chance of intravascular injection in this zone, and most experienced injectors prefer it here for that reason.
Why Does Forehead Filler Require a Different Logic Entirely?
The forehead presents an almost opposite anatomical challenge. The supratrochlear and supraorbital vessels travel upward from the orbit and run in relatively predictable planes above the periosteum before branching into the subdermal layers. Injecting at mid-depth — into the frontalis muscle or the submuscular plane — puts these vessels at direct risk of compression or cannulation.
Periosteal placement, deposited directly against the bone, keeps the product below the critical vascular layer. This is why forehead filler is categorically different from nasolabial filler in its technical demands: the bone is not merely background anatomy here, it is the target plane.
Forehead filler placed at the wrong depth is not simply less effective — it is actively more dangerous. The periosteal approach is not a stylistic preference; it reflects where the anatomy allows safe volume to sit.
Forehead cases also require careful assessment of the temporal vessels and the hairline zone. Volume placed too laterally or too superficially near the temples can compress branches of the superficial temporal artery, a complication with serious visual implications. This is one reason forehead filler should be considered a high-skill, high-consequence procedure rather than a routine augmentation.
Does This Mean Cannulas Are Always the Right Tool?
Not universally, but in both the nasolabial and forehead zones, blunt-tip cannulas reduce the mechanical trauma to vessels compared with sharp needles. The cannula cannot eliminate vascular risk — a pressurised injection through any instrument can still cause intravascular occlusion — but it substantially reduces the likelihood of direct arterial puncture. Cannula length, flexibility, and gauge are selected per zone, not interchangeably.
How Anatomy-Guided Planning Changes the Outcome
Approaching filler as a zone-by-zone product decision — “what volume for the nasolabial fold, what volume for the forehead” — is a less complete framework than mapping each area against its fat compartment architecture, the underlying bone structure, and the vascular territory involved.
In practice, this means a physician may look at a patient presenting with nasolabial folds and conclude that the primary deficit is in the mid-cheek fat, not the fold itself, and that placing filler medially would give a worse result than restoring lateral and deep cheek volume. Similarly, a patient concerned about forehead hollowing may need assessment of the temporal hollow and brow position before any forehead product is planned — because what reads as a forehead volume problem is sometimes a brow descent problem, which filler alone does not correct well.
This kind of layered assessment is what separates placement strategy from product placement. For a fuller explanation of how Tune Clinic structures this decision process, see the physician-led design method and our overview of facial filler at Tune Clinic.
FAQ
Is nasolabial filler dangerous compared to forehead filler?
Both zones carry vascular risk, but the risk profile differs. The nasolabial area involves the facial artery and its branches; the forehead involves the supratrochlear and supraorbital vessels. Neither zone is categorically more dangerous than the other — the risk in each depends heavily on injector anatomy knowledge, depth selection, and technique. Cannula use and aspiration practice reduce but do not eliminate risk in either area.
Why does filler placed directly into the nasolabial fold look worse over time?
Direct fold filling stiffens the crease rather than restoring the underlying volume that caused it to deepen. Because the nasolabial fold moves with every facial expression, product placed superficially within it is subjected to repeated mechanical stress, which can accelerate migration and distortion. Addressing the fat compartment deficit that underlies the fold typically produces a more natural result with less long-term distortion.
What depth should forehead filler be injected at?
The standard anatomically safe plane for forehead filler is the periosteal layer — against the bone, below the muscle and the neurovascular structures that travel above it. Placement at mid-depth within or above the frontalis muscle increases the risk of compressing or entering supratrochlear and supraorbital vessels, which can have serious consequences including skin necrosis or vision changes.
How do I know if I need nasolabial filler or cheek filler?
In many cases the answer is cheek or mid-face volume restoration rather than direct nasolabial filling. As the deep medial cheek fat and the nasolabial fat compartments deflate with age, the nasolabial fold deepens as a consequence. Restoring volume to those underlying compartments often softens the fold more naturally than filling the groove itself. A structural assessment by a physician — not a consultation focused on the fold in isolation — is the appropriate starting point.
Can nasolabial and forehead filler be done in the same session?
Yes, in many cases they can. However, the decision depends on the total volume being placed, the patient’s vascular anatomy as assessed during consultation, and the physician’s judgment about cumulative swelling and the ability to monitor outcomes across zones simultaneously. Some physicians prefer to stage high-risk zones across separate sessions to allow cleaner assessment of each result.
Ready to plan your treatment?
Tune Clinic Apgujeong offers English-language consultations with Dr. Ju and Dr. Cha — a structured assessment, not a sales call.
→Book an appointmentto pick a time that fits your Seoul itinerary.
→Message us on WhatsAppto ask in English before you commit.
