

On this page

Rejuran (PDRN) and dermal fillers solve different structural problems. Filler restores lost volume in soft tissue compartments; Rejuran works inside the dermis itself to stimulate fibroblast activity, rebuild collagen architecture, and improve the textural quality of skin that volume replacement cannot address. Confusing the two leads to treatment plans that overcorrect volume while leaving the underlying skin quality unchanged.
Why Don’t Fillers Fix Fine Lines?
Fine lines in the crow’s feet zone and around the mouth are not primarily a volume problem. They originate in the dermis — specifically in the loss of collagen density, elastin integrity, and the skin’s capacity for self-repair at the papillary layer. Adding volume to the surrounding compartment changes the contour, but the skin sitting above it remains the same: thin, less elastic, and structurally compromised.
This is a meaningful clinical distinction. A patient who receives temple or cheek filler may look less hollowed, yet the fine crepey texture across the lateral orbital area persists untouched. The two issues coexist, and they require separate tools.
Volume replacement lifts the scaffold beneath the skin. It cannot remodel the skin itself. When patients notice that something still looks “off” after a full filler treatment, the answer is often skin quality, not contour.
What Does PDRN Actually Do?
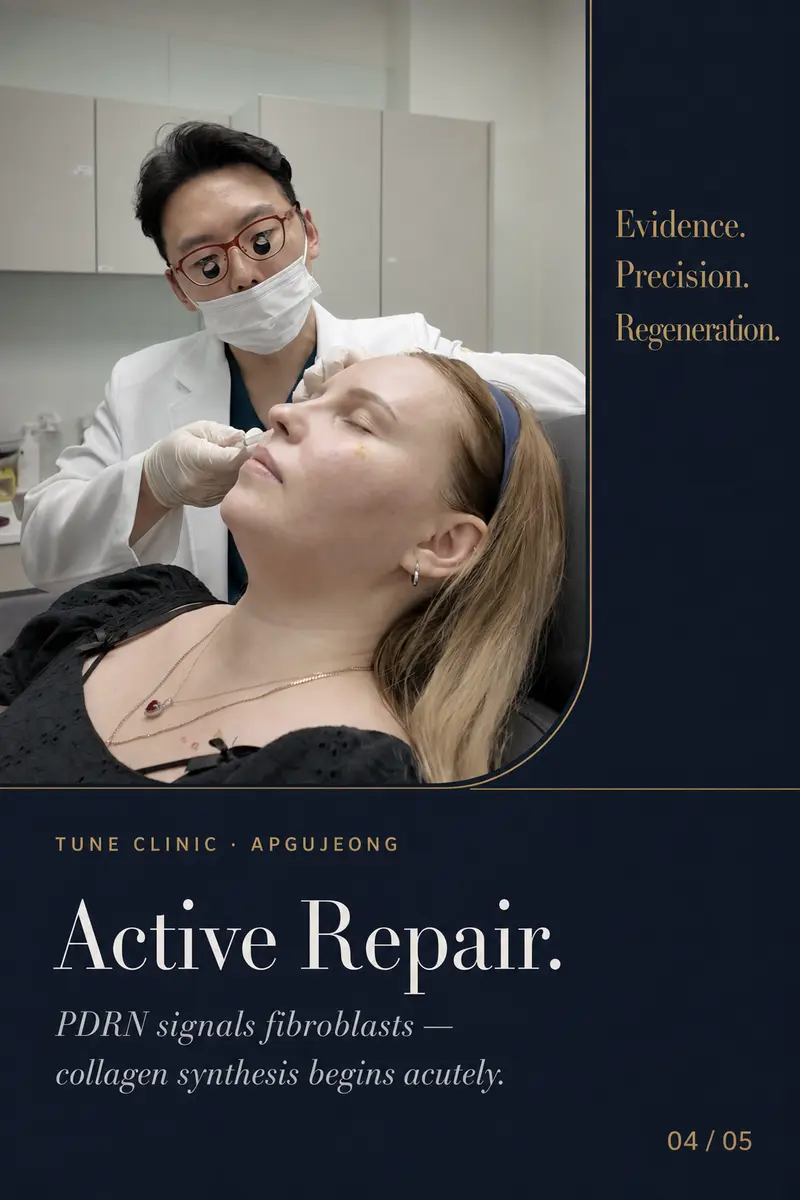
PDRN — polydeoxyribonucleotide — is a purified polynucleotide derived from salmon DNA. At the cellular level, PDRN binds to adenosine A2A receptors on fibroblasts and endothelial cells, triggering a cascade that promotes collagen and elastin synthesis and supports tissue repair. Clinical experience and published research both support its role in improving dermal density, fine-line depth, and overall skin quality over a course of treatment.
Rejuran is the brand most clinicians in Korea associate with standardised, pharmaceutical-grade PDRN, available in formulations including Rejuran Healer (for general dermal remodelling), Rejuran HB (with added hyaluronic acid for hydration), and Rejuran S (a more viscous formulation suited to deeper folds). The choice of formulation is part of the physician assessment, not a default.
Delivery Matters as Much as the Product
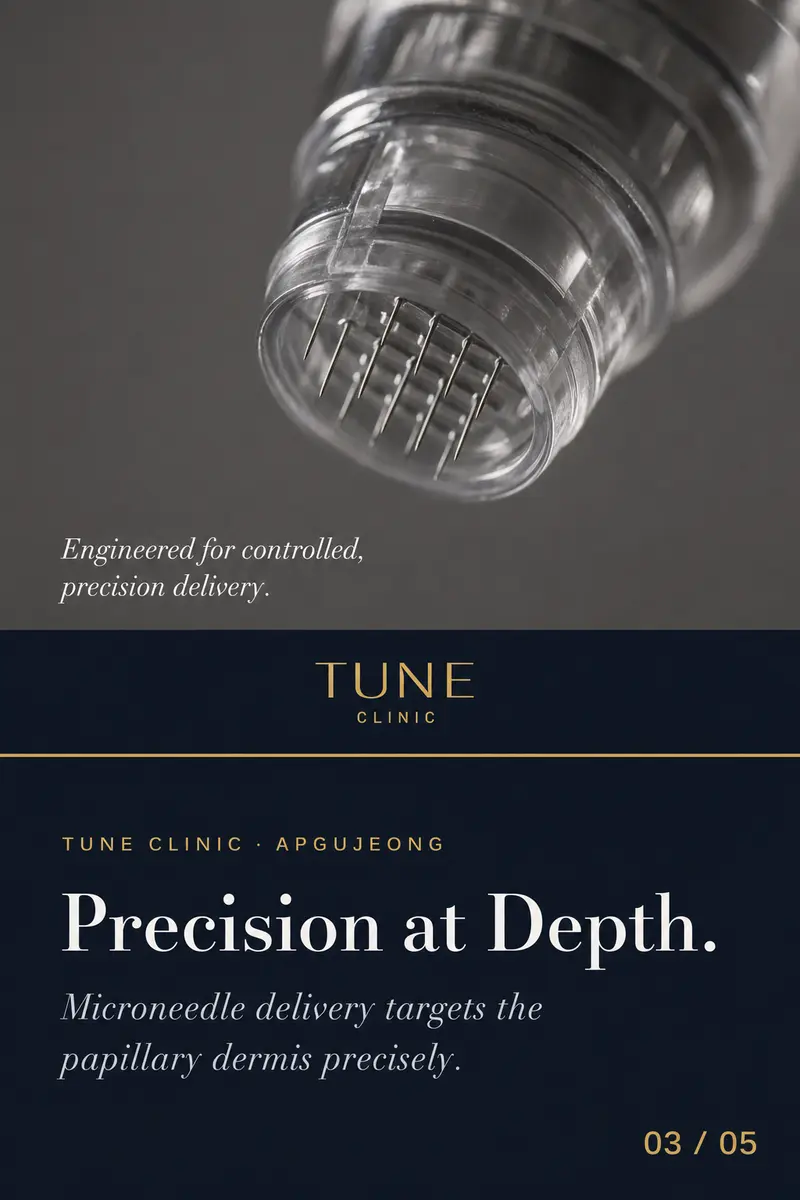
The papillary dermis — the uppermost layer of the dermis, just beneath the epidermis — is where fine-line formation occurs and where PDRN has its primary effect. Achieving consistent placement at that depth across irregular terrain like the periorbital zone requires precise microneedle delivery and a clinician who understands the anatomy of each sub-zone. Too superficial and the product disperses; too deep and the signalling effect is displaced from where the structural deficit actually sits.
Which Zones Respond Best to Rejuran?
In clinical practice, the areas that tend to show the clearest response to PDRN treatment are those where skin quality — rather than volume loss — is the dominant concern:
- Crow’s feet and lateral orbital area — Dynamic fine lines here are driven by thin, sun-damaged skin, not volume deficit.
- Perioral lines — Vertical lip lines and the surrounding skin lose collagen density with age and sun exposure; volume in the lips does not address this.
- Neck and décolletage — Skin in these zones is often neglected and responds well to repeated PDRN sessions.
- Overall facial skin quality — Diffuse crepiness, loss of glow, and reduced elasticity across the full face benefit from a broader treatment approach.
Not every patient presenting with fine lines is a straightforward Rejuran candidate. Some perioral lines have a significant volume component; some crow’s feet would benefit from neuromodulator treatment first. A physician assessment should determine the relative contribution of each factor before a protocol is designed. For patients where both skin quality and volume loss are in play, Rejuran and filler can be used as complementary tools — but they should be prescribed with clarity about what each is doing. See how the clinic approaches combined treatment planning at /design-method.html.
What Is the Treatment Course and Timeline?
PDRN works through a biological repair process, not an immediate volumising effect. Patients should not expect to see results the day of treatment. In clinical experience, most people begin to notice improved skin texture and a reduction in fine-line depth after two to three sessions, with a typical initial course of three to four sessions spaced two to four weeks apart.
Maintenance frequency varies based on the individual’s baseline skin quality, age, and lifestyle factors including sun exposure. Some patients maintain results with quarterly sessions; others return every six months. These intervals are determined in follow-up consultation, not set arbitrarily.
Post-treatment, mild redness and small papules at injection sites are expected and typically resolve within 24 to 48 hours. There is no meaningful downtime in most cases, though individual responses vary.
For patients considering whether Rejuran fits alongside an existing treatment plan that includes filler, the relevant questions are about anatomy and skin quality — not which products to combine for the sake of combining. More on the clinical logic behind injectable planning is available at /the-composition.html.
FAQ
Is Rejuran the same as a filler or skin booster?
No. Rejuran is a PDRN-based injectable that works by stimulating the skin’s own repair mechanisms — specifically fibroblast activity and collagen synthesis — rather than adding volume or hydration through a foreign substance. Skin boosters typically deliver hyaluronic acid to improve hydration and plumpness; Rejuran’s primary mechanism is biological signalling for structural repair, which makes it suited to fine-line correction and dermal remodelling rather than volume or surface glow alone.
How many Rejuran sessions are needed to see results for fine lines?
Most patients see meaningful improvement in skin texture and fine-line depth after two to three sessions, with a standard initial course of three to four treatments spaced roughly two to four weeks apart. Because PDRN works through a gradual biological repair process rather than an immediate physical effect, results develop progressively and continue to improve for several weeks after a course is completed.
Can Rejuran be combined with filler in the same treatment plan?
Yes, and in many cases the two are complementary — filler addresses volume loss in deeper structural compartments while Rejuran improves the quality of the skin itself. However, they should be selected as separate tools for separate problems, not combined by default. A physician assessment is needed to determine which issue is primary before any protocol is designed.
Is Rejuran suitable for the crow’s feet area?
The crow’s feet zone is one of the areas where Rejuran tends to perform well, because fine lines there are primarily a skin-quality and collagen-density issue rather than a volume deficit. Precise microneedle placement at the papillary dermis level is important given the thin, delicate skin in that region, which is why clinical technique matters as much as the product itself.
Does Rejuran treatment hurt, and is there downtime?
Injection discomfort varies by zone and individual sensitivity, but the periorbital area is generally more sensitive than other parts of the face. Topical anaesthetic is applied beforehand to reduce discomfort. Post-treatment, small papules or mild redness at injection points are normal and typically resolve within 24 to 48 hours; most patients return to normal activity the same day.
Ready to plan your treatment?
Tune Clinic Apgujeong offers English-language consultations with Dr. Ju and Dr. Cha — a structured assessment, not a sales call.
→Book an appointmentto pick a time that fits your Seoul itinerary.
→Message us on WhatsAppto ask in English before you commit.
